How Nurse Managers Can Use Data to Quantify Their Work
Guest article by Tim Darling and Joel D. Ray, MSN, RN, NEA-BC
To help nurses and nurse managers communicate most effectively with other departments, we propose that they lean into the language of data as it is used by other departments. In this article, we share an example approach with some newly available data that can support nurses and nurse managers as they talk to finance. We also share some examples of how and when they can request data from other departments to increase the fruitfulness of the dialogue.
The challenge for nurses and nurse managers today
Patients and families have their own set of languages: multiple spoken languages as well as body language and emotional languages. Nurses are incredible at moving between different patients and families and meeting them where they are in the language that they speak. Nurses do this through a language of their own that is grounded in connection, compassion, and caring.
Today, nurses are also increasingly exposed to the languages of many other functions in the health system.
- Patient experience. The language of surveys, survey scores, benchmarks, trends, and the implications of it all.
- Quality. The language of clinical data, such as nurse-sensitive indicators and infection rates, acronyms like CLABSI and CAUTI, and quality processes such as Value Stream Mapping and LEAN.
- Finance. The language of incremental overtime and team productivity, which includes nurses of all levels hearing the cryptic terms of budgeting and “Hours Per Patient Stay,” “Hours Per Workload Index,” FTEs, and non-productive time.
- Human Resources (HR). The language of employee engagement, staffing, headcount, retention, and time to onboard.
- Information Technology (IT). The language of reducing cost and complexity in the management and integration of systems and platforms.
- Patient transport, food, and environmental services. Nurses today need to coordinate with these colleagues about shared objectives, such as the timing of food for diabetic patients and the timing of discharge processes to maintain patient flow.
These languages are not anchored primarily in the patient-based values of connection and caring – they are anchored in data, process, cost management, and return on investment (ROI)-based decision-making. When nurses and members of other professional disciplines communicate, it can seem like they are talking across each other because they often have different objectives and speak different languages.



The breadth of the languages of other disciplines is even more relevant to nurse managers who have to coordinate and advocate with other leaders on a regular basis. Consider this scenario: an RN leader proposes the need for a new position without applying a business case rooted in clinical and finance taxonomy. While patient safety may be the appropriate and valid clinical implication for the request, building a case solely on the argument that “it’s a safety concern” can create an adversarial exchange with the finance department. This unintentionally sends a message that one either cares about keeping patients safe or saving money in an environment where both are necessary. Understanding and appreciating different perspectives is key to fostering a more empathetic and open-minded approach in our interdepartmental discussions.
Data is the universal language that allows nurses and nurse managers to present and defend paths of action in a way that aligns with other leaders. Nurses are naturally data-oriented in their decision-making, but they are less often fluent in the type of data spoken by other departments. When nurses talk about staffing ratios to justify an investment in additional team members, for example, they are speaking in terms that may not be clear to other leaders, leading to miscommunication and mutual frustration.
The language of data is direct and difficult to dispute, leveling the playing field for everyone in the conversation.
For example, when a nurse manager talks to a patient transport manager about the need for successful discharges at 10:00 AM daily, the patient transport manager may have no incentive to prioritize this request. However, nurses who bring finance and patient transport leaders together and share the financial savings of reducing Length of Stay (LOS) on the unit with successful early discharges may achieve interdisciplinary prioritization.
These inter-departmental discussions not only address immediate concerns but also have the potential to spark innovative ideas. For instance, they may lead to more effective ways of moving patients through to discharge, such as spacing or timing planned discharges or communicating discharge potential and readiness in a manner that complements, rather than conflicts with, the workflows of other vital departments in the discharge process. This potential for innovation and improvement should inspire and motivate us to embrace interdepartmental collaboration.
A new report, Quantifying Nurse Manager Impact, a co-publication between Laudio Insights and the American Organization of Nurse Leaders (AONL), presents an analysis from a three-year longitudinal study of 3,000 nurse managers and their team members in over 50 acute care facilities and many ambulatory locations nationally.
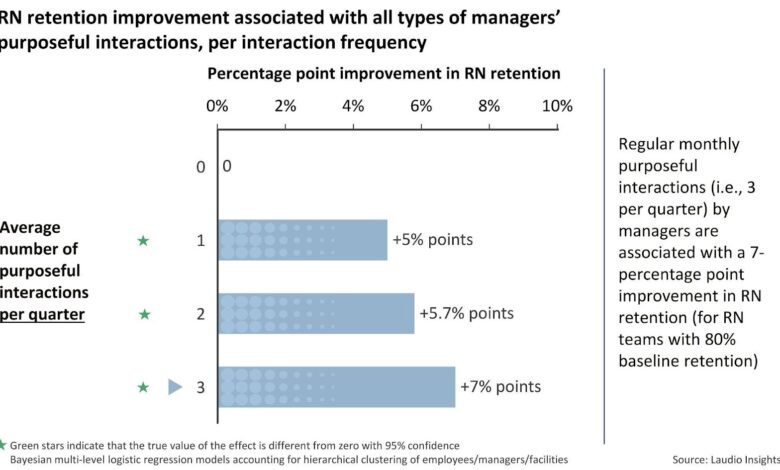
One of the key findings in the report was that inclusive of all sites of care and specialties, there is a statistically significant association between managers’ consistent, purposeful interactions with their team members and increased odds of RN retention (with 95% confidence). This highlights the powerful impact managers can make on employee retention – a major financial priority for both finance and HR leaders.
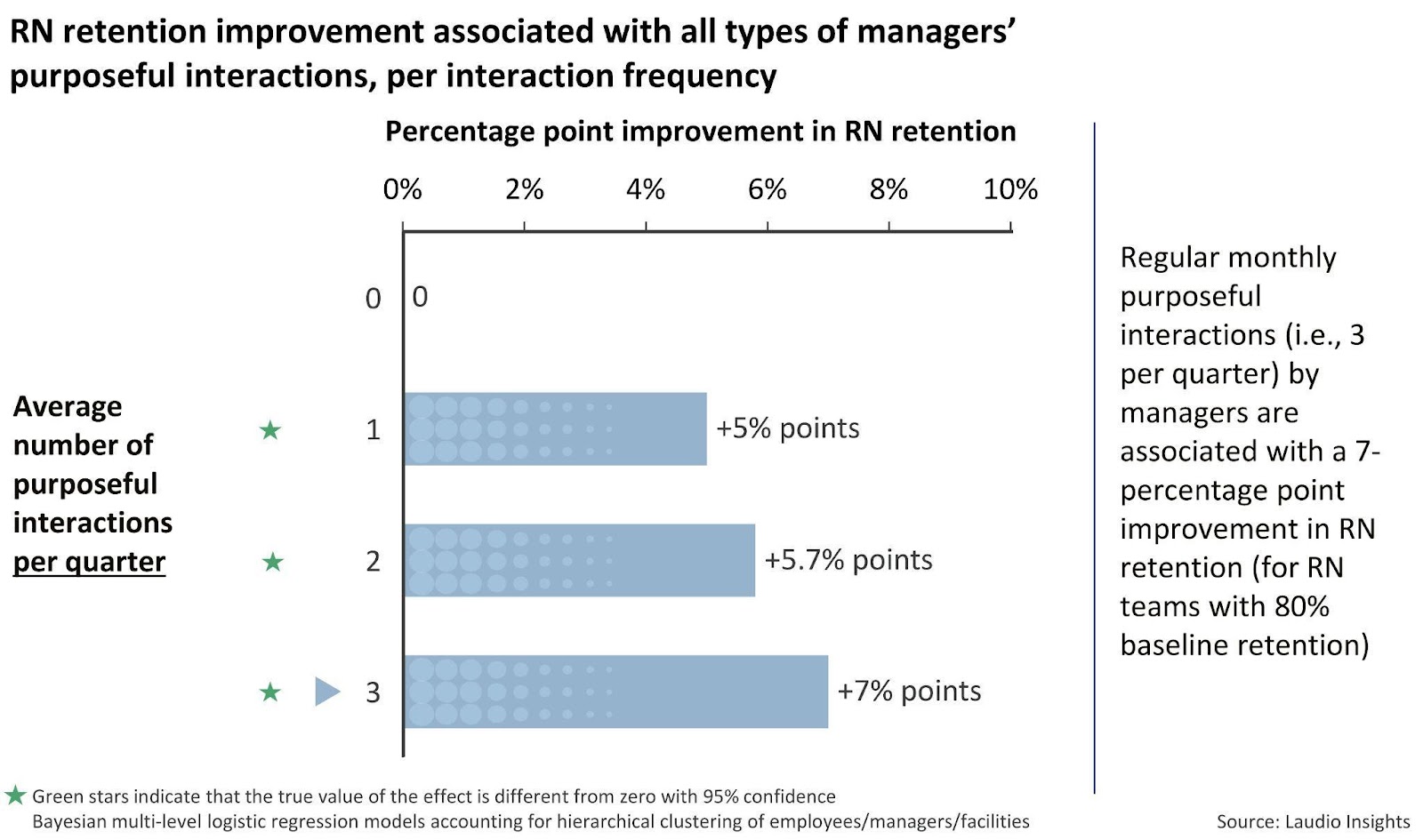
This chart shows the improvement in retention for a team of RNs with a 20% baseline annual turnover rate (values are calculable for other baseline rates; see the report for more details). As indicated above, introducing one meaningful interaction per team member per month for a year is associated with a 7-point decrease in turnover, with a resulting rate of 13%. For a hospital with 1,000 RNs, this equates to 70 RNs saved every year; a savings of $3.9M in replacement costs avoided, assuming an average $56,300 cost per RN turnover event (NSI 2024).
With high spans of control, elevated overall levels of responsibilities, and compounding administrative requirements, nurse managers today rarely have the time to connect with and maintain these levels of team interactions. Therefore, this data can help managers advocate for clarity of priorities, improved team design, reduction of administrative work, and new technology (e.g., self-scheduling and recognition tools) needed to reach these objectives – leveraging an ROI-driven justification for related investments.
By connecting the data and insights in the chart above with the language of financial impact, nurse managers can advocate for themselves and their teams with leaders of other functional areas, particularly HR and Finance. Leveraging data might require an adjustment in nurse managers’ communication styles as well as additional financial acumen, but it can fundamentally change their ability to advocate for needed resources, support, and tools.
Nurses might consider an ongoing dialogue with the finance department, building a language bridge that joins the two disciplines in meaningful discussion versus interacting only when a need becomes serious or “unsafe.” Asking finance partners about the essential financial indicators to understand and apply when case building for additional resources will help build the communication bridge and allow nurse leaders to rigorously advocate for resources.
Nurse leaders might also partner with finance to create small educational modules that help nurse managers build a common clinical finance language, allowing more efficient use of manager time and resources and translating into significant savings for the organization.
Data in action: How nurses can request and use data from other departments to inform clinical decision-making
In recent years, healthcare organizations have moved along a data continuum from being “data-rich and information-poor” to “information/analytics-rich but decision-making-poor.”
In order for a healthcare organization’s nurse managers to consistently engage in ROI-based decision-making, they need access to data not only at the organizational level but also at their unit level. Many organizations have not built the partnerships between clinical and financial leaders necessary to identify the necessary data for a nurse manager to make informed decisions when trying to balance quality and cost.
For example, investing in assistant nurse managers has been shown to have an impact on improving team member retention. Nursing managers can help inform these investment decisions if they have the data and are conversant in the data language of finance leaders.
Even when available to finance leaders, the information for key ROI data points, such as the cost of nurse turnover and Hospital Acquired Conditions (e.g., CLABSI, CAUTI, or falls with injury), may not be proactively shared with nurse managers. National data rarely carries the same weight in decision-making as actual costs specific to the organization.
Hospitals and health systems should commit to facilitating coordination between finance and nursing to build a shared, mutually agreed upon set of local costs that support ROI-based clinical decision-making. The result will be nurse managers who not only share the same goals as the larger organization but also speak the same financial language for data-driven decision-making as their colleagues in finance.
Nurse managers are the fulcrum through which the vast majority of a hospital’s strategic and financial goals are achieved. Nurses and nurse managers already speak many languages, such as the languages of compassion and clinical competence.
Now is the time for healthcare organizations to develop and empower their teams with a shared language of data-driven, financially grounded, ROI-based decision-making – with nurse managers and their team members providing a critical voice in the decisions that drive organizational success.
About the Authors
Tim Darling is a co-founder of Laudio and President of Laudio Insights. With over 20 years of experience in healthcare technology, Tim has a real passion for using data and analytics to serve the challenges facing healthcare organizations. The analytics and research arm of Laudio, Laudio Insights provides unique, evidence-based perspectives on dynamics affecting healthcare’s frontline workers and their leaders.
Joel D. Ray, Colonel (Ret.), USAF, NC, MSN, RN, NEA-BC serves as the Chief Clinical Advisor at Laudio. He has over 40 years of nursing and health system management experience. Previously Joel was the Vice President of Patient Care Services and Chief Nursing Officer at UNC Rex. Prior to UNC Rex, he served 26 years in the United States Air Force Nurse Corps, retiring with the rank of Colonel.

